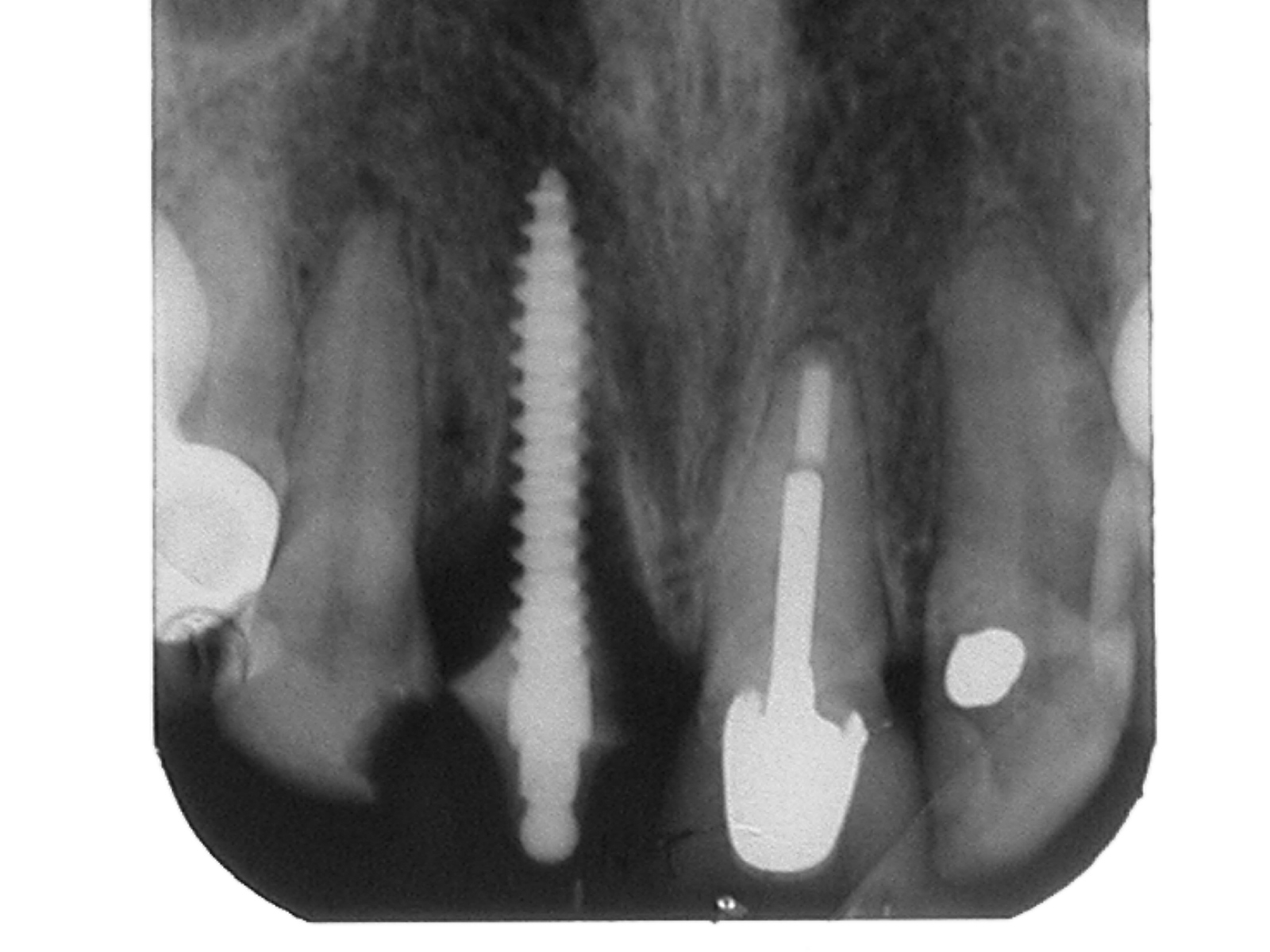
The most distal mini seems to be hitting the IDN. However, because of the small diameter of the mini, little damage is done and most of the time, it is asymptomatic. If symptoms occur, it is a simple matter to remove the mini and the nerve recovers rapidly. Severance or neurometsis of a nerve by a mini is almost impossible, and this is a hugh advantage over conventional sized implants. In this particular case, the xray probably shows an overlap rather than an impingement onto the nerve. There was no sign or symptoms in this case. Thus, a long mini can usually be used even if it seems to enter the nerve canal because it is often only apparent and even if it does so, the nerve is not injured because the nerve occupies only part of the canal and you have to be pretty "lucky" to strike it right in the centre.




Using the Buddy System as described in this blog, we placed mini implants and cemented on the buds. Immediately, we took an impression and sent it to the lab.
And two weeks later........... we cemented the bridge in and the patient went off.

More than a month later, the patient came back. No problems.... he was able to eat quite well on the right side. Can you now look at my left side.... the upper bridge is failing.... please do what you did like on the right side !!
The following pictures is another case of a free end saddle restored with minis.





This is the condition of the composite abutments around the mini-implants and its surrounding soft tissue 3 years later. The PFM bridge came off and had to be recemented. The soft tissue looks healthy and relatively inflammation free. This patient also happens to be a norcturnal bruxer.